


This goes for health and mental health practitioners—as much as it does for everyone, including you and me.
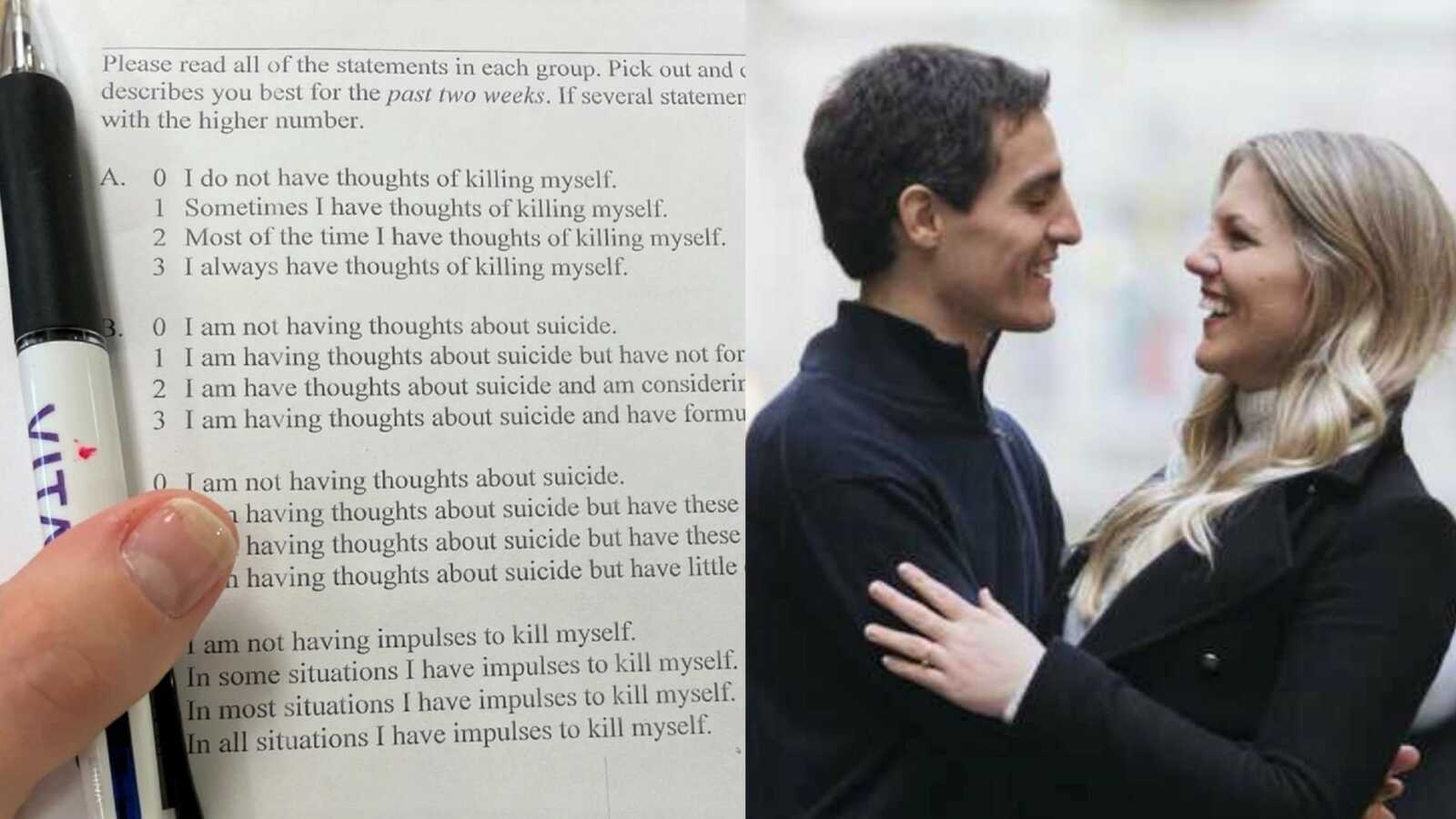
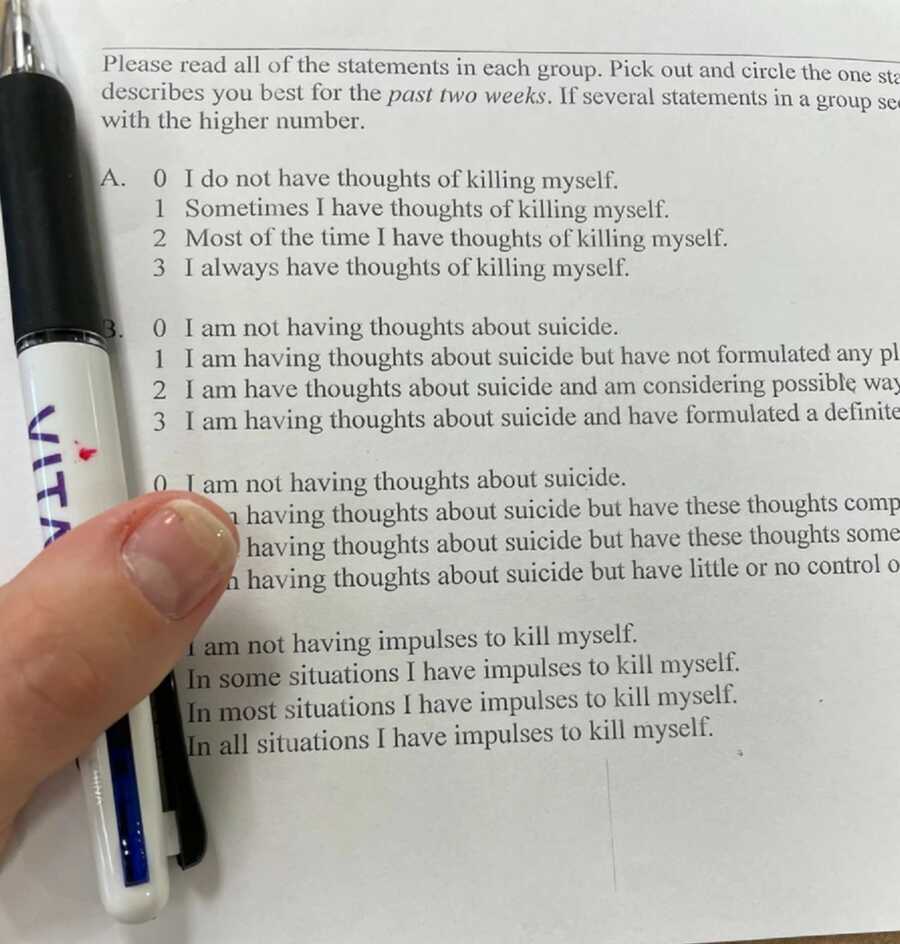
This morning I had my annual physical exam. For the first time that I can recall, my general practitioner’s office gave me a mental health screening—including an entire form on suicide. As a recent young widow by suicide loss (my husband took his life in 2020), the deceptively simple sheet of paper conjured visceral emotions and deep reflection.
I’m ecstatic that mental health is being integrated into regular healthcare. Doctors are a key player in initially identifying, and later treating, mental health issues. That said, I’m not convinced these sheets of paper adequately capture the presence of mental health conditions—especially the more “shameful” (read: stigmatized) ones.
As I filled out the form, I caught myself downplaying my own experience. For one, the delivery of the questions was frigidly cold; neither the words on the form nor the receptionist who handed me the sheet of paper gave me any sort of forewarning or comfort. I had no idea I’d be asked to disclose the deepest depths of my mental health—or life.
I’m not concerned I’m at risk for self-harm (although, as most widows and survivors of suicide loss will confirm, it’s crossed our minds at least once). I see a therapist weekly and prioritize my mental health. I meditate daily and have a regular spiritual practice, as well as take care of my physical body. I’m also a social worker myself. Regardless, I have bad days, some of them excruciatingly low. (Of course I do; my husband took his life.)
Yet as I filled out the form—I was compelled to share none of this. Instead of feeling supported in disclosing my mental health history, I felt defensive. Called out by the form. Turned off by its questions. Ashamed. As I looked over the questions, particularly those on suicide risk, I reflected on my husband.
How would someone who’s actively thinking about taking their life react to these same questions? How about a man like my husband, who’s living with hidden depression and complex PTSD caused by child abuse—someone who has no idea his past is linked to his current pain, yet blames himself for all of it?
According to a recent study funded by the National Institute for Mental Health (NIMH), about half of the men who die by suicide see their general practitioner one month before they take their life. This could be because they innately feel that something’s not right, and/or because they’re having somatic demonstrations from the stress of suicidal ideation.
At least the latter was the case with my husband. One month before his first suicide attempt, a terrible throat infection landed him in the hospital for three days. To the best of my knowledge, his mental health was not discussed while he was in the hospital. If it was, it didn’t interrupt his suicidal ideation and planning.

We’ve Got To Talk About Shame
There’s no panacea in treating mental health, but there’s one thing that can’t be denied: We’ve got to break down the shame behind it. This relates to the shame around feeling badly in the first place, and the embarrassment we may experience in asking for help. It also relates to the shame of why we need help—meaning the shame around what has happened to us, that causes us to feel depressed, anxious, and so on.
How do we break down these layers of shame? How do we make people feel safe sharing their most vulnerable selves, so they may access the help they need?
The solution, in part, hinges on normalizing shame’s various dimensions. It’s only by allowing people to feel safe and unjudged in sharing their stories, that they will open up and consider seeking help.
First, we’ve got to normalize feeling bad and seeking help for it.
Thanks to Instagram and the like, we live in a culture that mixes toxic positivity (“good vibes only!”) with unattainable ideals (“living my best life!”), alongside a heavy dose of glamorizing the grind of (over)working. Taken together, the message we receive is: Must. Feel. Good. Always. And if I don’t? Keep going. Or fake it.
Thankfully, there is pushback against these ideals, including on social media (ironically, one of the contributing factors to why we feel so bad in the first place). Especially among Millennials and Gen-Z, it’s now acceptable (and increasingly popular) to share personal stories of battling trauma, depression, anxiety, suicidality, and other mental health conditions; and share the ways we’re moving through it. (As it turns out, I’ve become one of these people.)

Yet while the tides of speaking truth on mental health are turning, we’ve still got a ways to go.
It takes time to get to a place where we’re comfortable acknowledging our painful experiences—even if only to ourselves. What’s more, many people (especially those in the throes of their trauma, like my husband) will never choose to turn to social media to process their understanding. Even seeking insight from others may be too much. Other people’s stories may hit too close to home and we may not be ready to read those words. Or, the world of mental health may feel so foreign we’re unsure where to go to find comfort and community.
Nevertheless, there is a shift taking place in talking about mental health. It will take time until this becomes an all-out norm, but we’re heading in the right direction. It’s only by allowing people to feel safe and unjudged in sharing their story, that they will open up for help.
Second, we have to normalize why we feel bad. This often stems from hidden trauma.
Aside from normalizing how we feel, we also need to normalize why we feel that way. What happened to us? What shadows haunt us from our past? It’s here that our darkest pain lives, and it’s here that the core of mental health conditions often lurks.
In March 2021, a year after losing my husband, my colleague and dear friend, Dr. Maria Piñeros-Leaño, and I gave a talk at Harvard Medical School on the issue of mental health. We focused on the Latinx community and specifically, on Latino men (which my husband was). Around 130 doctors, psychiatrists, psychologists, nurses, social workers, as well as students and faculty, joined us for a raw and honest discussion, which touched on the issues of trauma and shame.

One of our key takeaways was that in order to fully understand and alleviate mental health conditions, we can’t just look at the here and now. We also need to look at experiences from earlier on in life—especially traumatic ones. These include issues like family dysfunction, poverty, and child abuse of an emotional, physical, and/or sexual nature.
Echoing other recent research, we suggested one straightforward and effective way for medical and mental health practitioners to identify traumatic experiences that underlie mental health issues is to administer an Adverse Childhood Experiences (ACES) screening to all patients.
Through ten short, direct questions, this validated tool identifies whether an individual endured certain traumatic experiences as a child or adolescent (a.k.a., “ACES”), and if so, how many. As the research demonstrates, the higher the number of ACES an individual has lived through, the more likely he or she is to experience negative health or mental health complications, including depression, anxiety, and suicidal ideation. Such complications may be externalized (demonstrated and made known) or internalized (kept hidden and buried deep inside).
As we suggested in our talk, there is great potential in this intervention strategy, given that the single greatest predictor of virtually every health and mental health condition is traumatic experiences endured early on in life. (It’s important to note the research is not saying everyone who experiences mental health issues endured trauma as a child. What it is saying is that those who did are at a higher risk of experiencing adverse outcomes later on. At the same time, given the high prevalence rates of ACES, traumatic childhood experiences are more common than we’d like to think.)
Breaking Down Shame
So, what does this all mean for breaking down shame?
Traumatic experiences tend to be shrouded in shame. Traumatic events violate the very core of our being. They crush our ego and break our heart. Oftentimes, they harm our body. They strip us of our power and leave us vulnerable without our consent. When trauma occurs, it means something has been done to us to make us feel terrible about ourselves deep within. The younger we are when a trauma occurs, as well as the more frequent and severe the traumatic occurrence, the more likely it is to negatively impact us—oftentimes for years to come.
To add insult to injury, when a trauma occurs, we tend to blame ourselves for it. We’re ashamed of what happened to us. We’re often consumed by anger toward ourselves—anger for having “allowed” the trauma to occur. In reality, however, there was no “allowing” of anything. Trauma is done to someone by someone or something else.
When we’re put in a situation that is dangerous, overwhelming, or humiliating, we do what we have to do to survive it. It’s only in the aftermath we wish we’d acted differently. We wish we’d pushed our abuser away. We wish we’d stood up for ourselves when we were bullied. We wish we’d responded in any other way. But we didn’t. We couldn’t have. The fact of the matter is, we instinctively did what we did so we could make it through the traumatic event. (This is where fight, flight, freeze, and fawn responses come into play.)
The catch is, unless our patterns of shame and self-blame are interrupted, these sentiments, as well as as the trauma driving them, continue to fester. It’s only by acknowledging the trauma that occurred and seeking help to alleviate it, that we can begin to break free of trauma’s hold.
Addressing Shame
I can’t help but wonder: If my husband had been asked the ACES questions, would he have been nudged just enough to open up about his traumatic past? Would the questions have sent a signal of, “You’re not the only one who’s lived through this?” Would they have led him to talk to someone? To ask for help? Or would he have read an ACES screening the same way I read the mental health form at my yearly check-up—cold and disconnected?

As with so many questions tied to suicide loss, I’ll never know the answer. Yet my sense is that effective screenings boil down to the direct delivery of a compassionate, relevant screening tool; and the presence of a supportive social context in which that tool is administered.
On a direct level, mental health screening tools must pose questions in a human-centered, compassionate, supportive way that normalizes stigmatized experiences from the outset. The message needs to be, “You’re not alone in your experience. You are not flawed for feeling how you feel, or experiencing what you’ve experienced. You have a right to get help. And you won’t be judged in asking for it.”
Overall, screening is an experience and a part of mental health treatment. It should be designed as such.
In a related vein, if screening tools are to be successful, they can’t address current demonstrations of mental health alone. We now know that earlier life experiences shape our present mental health. If we are to understand (and improve) how we feel today, we have to be willing to look at our traumas from the past.
On a broader societal level, there needs to be more discussion not only of mental health conditions but also the root causes of them. To truly understand mental health, we need candid discussions of the big issues that cause people harm. By this I mean society’s really hush-hush problems—the ones that break our hearts to think about, but are so much more prevalent than we’d like to believe… child abuse and neglect. Incest. Substance abuse. Parents’ mental health conditions. Domestic violence. And the list goes on.
These are difficult issues to talk about, let alone tackle. But if we’re not willing to touch on them as a society at large—what message does that send to the people who have survived them?
In my journey fumbling through widowhood and suicide loss, I’ve crossed paths with incredible people who are sharing their stories of surviving exactly these issues. In their words is profound insight on the ways in which their past shapes their current lives, as well as wisdom on how to end the kinds of trauma they’ve endured.
More attention needs to be given to trauma survivors and the stories they share. Their words offer raw explanation of society’s most taboo (yet shockingly common) problems—as well as ways to stop them.
This article was submitted to Love What Matters by Dr. Lenore Matthew. You can follow her journey on Instagram, Facebook, and her website. Submit your own story here, and be sure to subscribe to our free email newsletter for our best stories, and YouTube for our best videos.
Read Lenore and Bruno’s story:
Read more stories like this:
Spread awareness for suicide prevention. SHARE this important story on Facebook and Twitter.